Alabama death row inmate who stopped gas execution wants to stop other methods
N.C. advances plan to reopen Martin Co. hospital; Advocates, elected officials call for statewide siren system after 14 tornadoes touch down near New Orleans.

It's Friday July 17, 2026 and in this morning's issue we're covering: Alabama death row inmate who stopped gas execution wants to stop other methods, Eight school-based health clinics close in Southwest Virginia as federal funding pressures mount, The ‘Hub-and-Spoke’ Model for Addiction Treatment in North Carolina, Wildfire Smoke Is Back and Making the Air Unhealthy: Your Guide To Staying Safe in NYC, Repeated storms are turning disaster recovery into a way of life, and leaving communities facing disaster fatigue, NC auditor’s former liaison resigns amid furor over pressuring county elections board on early voting plans, State budget advances plan to reopen Martin County hospital, This county lost its hospital. Bringing it back is easier said than done, Advocates, elected officials call for statewide siren system after 14 tornadoes touch down near New Orleans.
Media outlets and others featured: Alabama Reflector, Virginia Mercury, The Daily Yonder, The City Reporter, The Conversation, Carolina Public Press, North Carolina Health News, Mississippi Today, Verite News.
Alabama death row inmate who stopped gas execution wants to stop lethal injection execution
By Ralph Chapoco (Alabama Reflector) Published: July 15, 2026
Attorneys for an Alabama death row inmate who successfully challenged Alabama’s nitrogen gas execution protocol last month have asked a federal judge to prevent the state from using a different execution method to put him to death.
In the July 7 filing, attorneys for Jeffrey Lee asked the U.S. District Court Judge Emily Marks to expand an injunction against nitrogen gas to lethal injection and electrocution, the state’s two other statutory methods of capital punishment. The filing said it would be “manifest injustice.”
“Mr. Lee would face execution by a method he specifically elected away and that the state represented he would not face,” the motion states.
SUBSCRIBE: GET THE MORNING HEADLINES DELIVERED TO YOUR INBOX.
Attorneys for Lee declined to comment further on Tuesday.
A message was sent to the Alabama Attorney General’s Office and the Alabama Department of Corrections on Tuesday seeking comment. The court has given Alabama until July 17 to reply.
Lee was convicted of the 1998 murders of Jimmy Ellis and Elaine Thompson during a robbery of a pawn shop in Orrville. A jury voted 7-5 to sentence Lee to life in prison, but the presiding judge overruled the jury and sentenced Lee to death. The practice of judicial override was abolished in 2017.
Lee was scheduled to be executed by nitrogen gas in June, but he argued that the method amounted to cruel and unusual punishment. Witnesses to prior nitrogen gas executions have reported those subjected to it struggling and gasping for air through the process. Lee said he would prefer to be executed by firing squad, a method not currently authorized by Alabama.
Marks in June ruled that while Lee would experience “air hunger,” the acute distress that people who are in the process of getting executed will experience, she ruled it was an “inescapable consequence of death” and not additional pain beyond what is needed to put someone to death.
On appeal, a three-judge panel at the U.S. 11th Circuit Court of Appeals reversed that part of the ruling, writing it was “over and above the mental distress that typically accompanies the knowledge of impending death by execution.” The panel directed Marks to determine whether execution by firing squad was feasible.
Marks ruled it was and enjoined the state from executing Lee by nitrogen gas.
The Alabama Attorney General’s Office immediately appealed that ruling, seeking a stay of the permanent injunction, but the 11th Circuit and the U.S. Supreme Court declined to overturn Marks’ ruling. The Alabama Attorney General’s Office then filed an expedited request with the Alabama Supreme Court, seeking to execute Lee by lethal injection.
Lee’s attorneys wrote in the July 7 filing that attorneys for Alabama in 2018 agreed to settle a lawsuit filed by Lee in 2016 against the state’s lethal injection protocol, after Lee opted into execution by nitrogen gas. Lee’s attorneys cited language in the agreement that an attempt to execute Lee would be carried out by nitrogen gas, and “not the three-drug lethal injection protocol at issue in this litigation.” That, they argued, prevented execution by lethal injection.
“Having secured dismissal of that action based on that representation, the state cannot reverse course,” the motion states. “Yet in seeking a new execution date for Mr. Lee after he prevailed in challenging the protocol, the state now asserts that it ‘is prepared to execute Lee via lethal injection with the three-drug cocktail adopted in 2014.”’
Lee also argues that the state cannot go back on its word.
“Mr. Lee reasonably relied on the State’s representation that his execution would be by nitrogen hypoxia, not lethal injection, and dismissed his lethal injection lawsuit as a result. Equity forbids the State from reversing on that representation to Mr. Lee’s detriment,” the motion states.
The motion argues that Alabama law states people can only be executed by lethal injection only if nitrogen gas is no longer available. That is not currently the case because “lethal injection is available only if nitrogen hypoxia as a method of execution—not merely the protocol implementing it—is held unconstitutional by the Alabama Supreme Court or the U.S. Supreme Court, or by the Eleventh Circuit if certiorari is denied.”

Eight school-based health clinics close in Southwest Virginia as federal funding pressures mount
By Charlotte Rene Woods (Virginia Mercury) Published: July 10, 2026
Federally Qualified Health Centers in Southwest Virginia have shut down eight school-based health clinics, prompting the Virginia Community Healthcare Association to urge U.S. Rep. Morgan Griffith, R-Salem, to intervene. The association, which represents FQHCs across the state, sent Griffith a letter Thursday about the closures.
The outreach program had served as an extension of health services into communities where access to primary care is limited. It has been funded by reinvesting savings from a federal drug pricing program back into the communities the clinics serve.
The federal program, known as 340B, allows qualifying hospitals and clinics that treat underserved populations to buy prescription drugs at steep discounts while charging insurers full price and keeping the difference.
The arrangement helps safety net providers that operate on tighter margins reinvest the savings back into their communities, including the school-based clinics that have since closed.
VCHA CEO Tracy Douglas wrote in her letter that the Southwest Virginia coalition of clinics had realized about $2.7 million in annual 340B savings, but those savings are projected to decline by $400,000 amid rising demand for care.
FQHCs are among safety net providers that also include free clinics and health-related nonprofits, all of which are facing growing demand as people lose health coverage amid various federal actions.
Simply put, it’s getting harder to stretch 340B dollars at a time when clinics are stretching everything.
Complicating matters are ongoing debates over the future of 340B.
After some hospital systems in Virginia and elsewhere were found to have improperly used the program, state and federal lawmakers have spent years exploring reforms to strengthen accountability, restrict how 340B is used and adjust how payments are made.
Reaction to the proposals has been mixed, with large pharmaceutical companies, pharmacies, hospital systems and smaller clinics like FQHCs offering competing views on how the program should be changed.
Outgoing U.S. Sen. Bill Cassidy, R-La., recently released draft legislation that FQHCs and other smaller clinics say could hurt them by changing reimbursement timelines, though broader reforms have drawn favorable responses from a variety of groups.
President Donald Trump’s administration also continues to pursue regulatory changes that would scale back the program.
“Because of the drama around the effectiveness of the program, we’re forced to have to make tough decisions,” Douglas said in a recent interview about the service cuts in Southwest Virginia.
The affected schools are:
- Northwood Middle School
- Saltville Elementary School
- Chilhowie Elementary School
- Chilhowie Middle/High School
- John S. Battle High School
- Highpoint Elementary School
- Virginia Elementary School
- Virginia High School
Calling the financial reality “stark,” Douglas said 340B savings had allowed the clinics to absorb the financial losses associated with operating the school-based health centers. Using 340B funds for that purpose, she said, is exactly what the program was designed to support. Douglas also recently participated in a roundtable discussion with Gov. Abigail Spanberger and representatives from Virginia hospitals, free clinics, state health agencies and health insurers.
With expired enhanced Affordable Care Act subsidies — though Virginia’s budget will help offset some of the impact for residents come November — and changes to Medicaid and hospital funding included in the federal reconciliation bill passed last summer, healthcare providers are warning lawmakers about mounting financial pressures and discussing ways to respond.
As thousands of Virginians lose or risk losing health coverage, providers expect greater demand for FQHCs, free clinics and hospital emergency rooms.
“What is happening in Virginia is very similar to what we know is happening in other states,” Spanberger said at the roundtable meeting earlier this week.
She emphasized that her administration is listening to providers and working to “look at how we can protect our vulnerable neighbors.”
SUBSCRIBE: GET THE MORNING HEADLINES DELIVERED TO YOUR INBOX.
The ‘Hub-and-Spoke’ Model for Addiction Treatment in North Carolina
by Taylor Sisk, The Daily Yonder
July 15, 2026
Holly Warren was recently leafing through one of her old medical school textbooks, trying to recall how much instruction she’d received in addiction medicine – trying to recall, “Did we even talk about this? Was it even on our radar?”
“And it really just wasn’t,” Warren said. She received an excellent education two decades ago at East Carolina University’s Brody School of Medicine, then at Duke University for internal medicine. “But we just really didn’t talk about addiction medicine very much.”
Today, Warren knows quite a bit about it. She began providing medications for opioid use disorder, or MOUD, at a federally qualified health center in rural Greene County, North Carolina, and now serves as medical director of the health department in Lenoir County, likewise a rural county in eastern North Carolina, where her clinical focus is MOUD.
She’s found support from the NC STAR Network.
In 2023, the federal Substance Abuse and Mental Health Services Administration lifted a restriction on health care providers’ ability to administer buprenorphine, considered a “gold standard” for treating opioid use disorder. Now fully capitalizing on this opportunity, the NC STAR Network is an initiative designed to expand access to addiction treatment for North Carolinians.
The network is a partnership of three hubs – the medical schools at the University of North Carolina at Chapel Hill and East Carolina University, and the Mountain Area Health Education Center, or MAHEC – and health care practices throughout the state. The objective is to train and support primary care providers to administer MOUD.
The network has received funding from the Foundation for Opioid Response Efforts, which cites it as a model of sound investment of funding from the Rural Health Transformation Program: $50 billion in federal money over the next five years to improve rural health care systems.
The Hub-and-Spoke Model
For Claire West, an internist in UNC’s Division of General Medicine and the NC STAR Network’s director, addiction medicine is the “absolute essence of primary care.”
“I think I speak for my colleagues in primary care, whether it’s family medicine or internal medicine,” West said, “that we were drawn to this because of our strong belief in whole-person care.”
Addiction is a chronic disease, she stresses, and should be treated in the continuum of whole-person care.
The NC STAR Network was built using a hub-and-spoke model, inspired by the approach the state of Vermont takes to addressing opioid use disorder. The medical schools and MAHEC serve as the hubs, offering a full range of care and training and support for the spokes, while the spokes provide ongoing care in a community setting.
The relationship between the hubs and spokes has continued to evolve.
“To remove the idea that the hub provides and the spoke receives was really important,” said Gabriela Castro, a family medicine physician in rural Chatham County and the NC STAR Network’s data team lead. “It’s bidirectional communication and learning,” with the community-based practices helping hub staff “understand what’s happening on the ground, what works for their specific community.”
The network now reaches into 88 of North Carolina’s 100 counties. From July 2024 to June 2025, the academic hubs provided MOUD to 1,400 patients, while spike sites reported serving well more than 4,000.
Every Door Open
The NC STAR Network team believes the primary care environment is ideal for administering addiction medicine for a number of reasons.
To begin with, “There’s a longstanding relationship; there’s trust, and there’s continuity,” Castro said. Delivering addiction medicine in the continuum of primary care “helps us frame the treatment of substance use disorder as one of many parts of a complex system of conditions that affect individuals.”
Moreover, she said, “Any door should be the right door when somebody wants treatment.”
Data indicate that patients who receive MOUD treatment in a primary care setting have equivalent retention rates as those who receive specialty treatment and often report greater satisfaction with the experience.
Embedding addiction medicine into primary care practices also helps destigmatize the treatment, Castro said.
“When we separate it from the rest of primary care, it becomes not only difficult to access but shameful for many patients,” she said. In a primary care office, “many patients feel much more comfortable; they’re already being seen for other conditions.”
The visit, West said, then offers her an opportunity to say to her patient, “‘I’m going to start giving you pre-exposure prophylaxis for HIV. I’m going to screen you and treat you for hepatitis.’ I can do all of these things.”
Or, to a patient who’s using methamphetamine, “‘You don’t want to stop using methamphetamines because you’re unhoused and you need to stay awake for your self-protection? I see that. I’m going to work with the case manager to help you find some housing resources.’”
Rural Reach
As has been widely reported, rural America has a shortage of most all health care services. This is certainly the case with the availability of MOUD. MAHEC is playing a critical role in addressing that.
MAHEC serves largely rural Western North Carolina. A primary objective is to place health care professionals in rural communities and provide them with the resources and training to remain there. Addiction medicine has been folded into that.
The Foundation for Opioid Response Efforts has invested in MAHEC’s role in the NC STAR Network. Karen Scott, the foundation’s president, said her organization found the network to be a sound investment not only because of its potential reach but the diversity of access points – MAHEC, the academic medical centers, local health departments, federally qualified health centers – allowing primary care practitioners throughout the state to tap into specialist expertise.

The MAHEC team, Scott said, has played a critical role in disseminating that expertise across rural Western North Carolina.
When Zach White, MAHEC’s opioid dependence treatment program coordinator, first started providing MOUD, a standard question he asked of new patients was, “Do you have a primary care provider?” And the most common response, he said, was, “No, but I’ve been meaning to get one.”
“We’ve got such a great opportunity, because, as we know, folks are coming in having used substances sometimes for many years and have not been tending to their health,” White said.
Foundation for Opioid Response Efforts program director Ken Shatzkes hopes to see other states looking to the NC STAR Network as a model for investment in the Rural Health Transformation Program funding. While the applications states have submitted for that funding don’t “explicitly say, ‘We need to build hub-and-spoke systems,’” he said, “the elements of what makes this a success are in those applications.”
‘Pretty Cool’
Acknowledging the treatment of substance use disorder as a chronic condition, Castro said, has transformed the way her primary practice addresses other conditions.
“It really helps us think about meeting the patient where they are,” she said. “We can’t push them too soon; we can’t push them any further than they want to go. We’re here to offer consultation and support and work with the logistical difficulties that they encounter navigating the health care system.”
“It absolutely has transformed the way I treat other things,” Castro said, “and I’m a better primary care physician.”
The NC STAR Network continues to expand its reach across the state.
Sandy Thomas-Montilus is an internist who provides MOUD in the rural southeastern region of the state, is clinical director of the N.C. Department of Adult Correction’s MOUD program, and is an NC STAR community partner. She stresses the importance of networking – networking that she believes can, in addition to expanding access to a critical treatment, help chip away at the stigma around addiction and addiction medicine.
“There’s still a lot of stigma amongst my own profession,” Thomas-Montilus said, “the idea that, ‘I don’t want those kinds of people in my practice.’ And to me, that’s very sad.”
Having played a role in the overdose crisis – some unaware of the addictive nature of prescription opioids; others through irresponsible prescribing, “I think we owe it to our patients” to be proactive in addressing it, she said. “The profession does.”
Holly Wilson says that when she was practicing primary care, her first objective was “for my patients to know that I cared about them. I couldn’t always fix their diabetes or their high blood pressure or various chronic conditions they faced,” she said, “but most importantly, I wanted them to know that I care.”
Now in addiction medicine, “I have to say it’s pretty cool,” she said, “to be able to continue to practice that primary objective, and to see lives pretty quickly changed by offering evidence-based care.”
“It’s really rewarding to see people heal and recover from a chronic illness.”
This article first appeared on The Daily Yonder and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.

Wildfire Smoke Is Back and Making the Air Unhealthy: Your Guide To Staying Safe in NYC
Canadian fires are lowering air quality in New York City … again. Here’s what to know.
By Kaitlyn Schwanemann, The City Reporter
Jul 15 5:00am EDT

With smoke traveling in from wildfires burning in Minnesota and Ontario, New York is due for a week of hazy skies and possibly poorer air quality.
New York City Emergency Management officials said Wednesday the smoke is making air quality “unhealthy” in some parts of the city, coinciding with dangerously high temperatures. They urged New Yorkers to limit outdoor activity, keep windows closed and wear masks when outside.
The entire state is under an air quality advisory for fine particulate matter pollution Wednesday due to the wildfire smoke, according to the state Department of Environmental Conservation.
https://twitter.com/nycemergencymgt/status/2077444727331332401?s=20
Thursday's forecast was not looking much better: Officials said an air quality advisory for the city would be in effect from 11 a.m. to 11 p.m.
When smoke from Canadian wildfires engulfed the city in June 2023, the boroughs turned suddenly orange, with air quality indices reaching 484 — the highest ever recorded. It may not get quite that bad in the city this time around, but the forecast can change quickly.
Experts told The City Reporter the smoke event could last for several days, and the smoke could get thicker and closer to the ground through Thursday — as yet another heat wave sets in. Here’s what else to know.
Jump to ...
- What Is an Air Quality Index, or AQI, and How Is It Measured?
- Is It Safe To Walk My Dog During New York’s Air Quality Alert? Is It Harmful To Exercise Outdoors?
- Will This Wildfire Smoke Hit New York as Hard as It Did in June 2023?
- Is My Indoor Air Safe? Can I Run My Air Conditioner?
- When To Stay Home and When To Call a Doctor
- Does an N95 Mask Protect Against Wildfire Smoke?
- When Will the Wildfire Smoke Leave New York?
What Is an Air Quality Index, or AQI, and How Is It Measured?
The air quality index, or AQI, is a metric used by the federal Environmental Protection Agency to gauge how much pollution is in the air, and how concerning it may be to human health.
When the AQI is between zero and 50, the air quality poses little or no risk to human health, but the higher the index, the more risk. The DEC and Dept. of Health and Mental Hygiene issue air quality health advisories when the AQI exceeds 100, meaning members of sensitive groups may experience adverse health effects. The risk at this point remains low for healthy people, but sensitive people should avoid strenuous and prolonged outdoor activities.
Sensitive people may include people with heart or lung conditions, people with weakened immune systems, adults aged 65 or older, pregnant people, infants and children with health conditions, and people with social vulnerabilities, such as limited access to housing, transportation or health care.
Healthy individuals aren’t usually affected by air quality until the AQI exceeds 150.
https://twitter.com/NYSDEC/status/2077399232571453728?s=20
You can check the AQI in your area by clicking here, a government-run air quality site. You can also find an air pollution map here maintained by IQAir, a Switzerland-based air quality technology company.
Due to ozone pollution unrelated to wildfire smoke, the New York City metro area was under an air quality health advisory on Tuesday.
Is It Safe To Walk My Dog During New York’s Air Quality Alert? Is It Harmful To Exercise Outdoors?
Smoke conditions can negatively affect pets the same as humans, according to guidance from the American Veterinary Medical Association. That group suggested that dogs (and cats) only go outside in short bursts to relieve themselves when air quality alerts are active.
If animals are experiencing coughing or gagging, difficulty breathing, eye irritation, weakness or other symptoms, you should call your veterinarian, they said.
As for taking a walk or exercising at the current AQI — under 150 — for healthy people, it’s safe to walk your dog, exercise outside and more. For sensitive groups and people more sensitive to air pollution, continue to monitor your symptoms, as you may experience heightened symptoms.
If the AQI exceeds 150, all New Yorkers should limit strenuous and prolonged outdoor activities. A short walk should be fine for healthy people, but avoid being outside for longer than an hour. If the AQI exceeds 200, all unnecessary outdoor activities should be cancelled or rescheduled, and the same goes for your pets.
“If you're sensitive to air quality, don't remain in a space without air conditioning or filtration. And if you're in a population vulnerable to heat — older adults, young children, people with chronic conditions — take the heat seriously, too,” the city's Emergency Management Commissioner Christina Farrell said in a press release Tuesday. “In both cases, you should get to a cool indoor space, and if you don't have one at home, a cooling center is open near you.”
To find a city-run cooling center near you, click here.
Will This Wildfire Smoke Hit New York as Hard as It Did in June 2023?
When Canadian wildfire smoke came to New York three summers ago, flights were grounded, public beaches closed and alternate side of the street parking was suspended. The AQI hit a record high, deeming the air unsafe for all New Yorkers, not just sensitive groups.
James Tomasini, a meteorologist from the National Weather Service, told The City Reporter that he’s not expecting it to be as bad — but he’s continuing to monitor the situation.
Amanda Lefton, commissioner of the DEC, said in a press conference on Tuesday that rain later in the week could help tamp down the smoke, but the situation is evolving and conditions depend on how well wildfire suppression efforts go in Minnesota and Ontario.
Is My Indoor Air Safe? Can I Run My Air Conditioner?
If the AQI becomes dangerous as wildfire smoke makes its way to the city, there’s a few ways you can protect your apartment from it.
The first step is to keep doors and windows firmly closed and sealed. You can stuff rags and towels against any cracks in doors or windows to block air and smoke from seeping in.
Most air conditioners are safe, because they cool down your apartment by circulating indoor air — not by bringing outdoor air inside. But make sure the filter is functioning properly, and clean.
The Environmental Protection Agency has more tips here on using an air conditioner during smoky conditions.
Run a high-quality air purifier, if you have one — and if you don’t, you can make a DIY version using air filters and a box fan. Some experts recommended purchasing air filters rated MERV-13 in bulk in advance of smoke events, so they’re ready to go when you need them.
When the AQI improves, ventilate your home and replace dirty HVAC and air purifier filters.
When To Stay Home and When To Call a Doctor
Every New Yorker has their own sensitivity to smoke and air pollution, but if you experience respiratory distress, seek medical help. If you have asthma, refill prescriptions for inhalers and other medications in advance. Click here for more tips on staying safe from the city’s health department.
Does an N95 Mask Protect Against Wildfire Smoke?
Yes, experts say that a tight-fitting, high-quality KN95 or N95 mask is a good defense against the particles distributed by wildfire smoke. Free masks will be available at public library branches across the city, including Brooklyn and Queens Public Library locations, and a few New York Public Library locations: St. George Library Center in Staten Island, the Bronx Library Center in The Bronx and the Stavros Niarchos Foundation Library in Manhattan.
When Will the Wildfire Smoke Leave New York?
Hazy skies were already visible in the city on Tuesday, but smoke was expected to come closer to the ground on Wednesday and Thursday, making visibility worse, Tomasini said.
It’s unclear exactly when the smoke will pass through the city as conditions are still evolving. Lefton said this is expected to be a “multi-day event.”
This article was adapted in part from The City Reporter’s previous coverage of wildfire smoke conditions from 2023.

Repeated storms are turning disaster recovery into a way of life, and leaving communities facing disaster fatigue
Increasing flash flooding is exhausting communities as they’re hit again and again.
By Lee Ann Rawlins Williams, University of North Dakota, The Conversation (The Conversation) Published: July 13, 2026
By Lee Ann Rawlins Williams, University of North Dakota
Flash flooding has been tearing up communities across the U.S., with heavy downpours sending creeks and rivers rushing over their banks from Texas to Kentucky, across the Midwest and into the Mid-Atlantic states and the Northeast.
Texas’ Hill Country was hit hard again when a powerful storm triggered flooding on the Guadalupe and other rivers on July 16, 2026, in the same region where more than 100 people, including young campers, died in flash flooding on July 4, 2025. In Missouri, floodwater swept away a home, and National Guard helicopters had to rescue and evacuate dozens of people from a summer camp.
If this feels like déjà vu after two summers of flash flooding across America, imagine being a community that has had to live through flooding like this again and again.
Residents in Cocke County, Tennessee, were still recovering from the effects of Hurricane Helene’s deadly 2024 rush of mountain floodwater when a new storm turned creeks into raging rivers in June 2026. Officials in Tioga County, Pennsylvania, had been lobbying the state to dredge flood-prone streams before flash flooding in early July 2026 hit the same communities flooded by Hurricane Debby’s remnants two years earlier.
As storms intensify in our warming world, recovery no longer feels permanent in places at risk of disasters. Instead, it’s too often a temporary reprieve before the next disaster hits. Communities are also spending down their savings to rebuild, and they’re finding bank accounts thin when disaster strikes again.
This state of repeated disasters is known as disaster fatigue. As a researcher who works on disaster planning and recovery, I’ve seen how this problem has grown for residents and communities at risk of fires, floods, hurricanes or other natural disasters.
When recovery never really ends
The traditional disaster response model assumes a sequence of preparedness, response, recovery and, eventually, a return to stability.
However, a full recovery from major flooding or a hurricane takes years. Increasingly, communities might not have completed repairs before another damaging storm arrives. At the same time, families rebuilding after a hurricane may confront a housing shortage. Insurance and reconstruction costs rise. Businesses and their workers face economic uncertainty about how soon they can reopen. Farmers recovering from drought may face another season of extreme weather before their livelihoods are restored.
The same pattern can be seen beyond weather-related disasters. In Venezuela, powerful earthquakes in 2026, followed by aftershocks, occurred within a broader context of economic and humanitarian challenges, making recovery even more complex.
In many places, recovery is no longer a destination. It has become an ongoing and seemingly unending process.
Emergency management scholar Victoria Ingham and colleagues define community disaster fatigue as the deterioration of the community’s ability to function, its well-being and its capacity to recover when disasters repeatedly disrupt daily life and overwhelm the community’s resources. Research examining communities exposed to repeated disasters has found evidence of fraying social networks and growing strain on the government and community systems essential for recovery.
Related research on resilience fatigue among residents suggests that repeated exposure to hazards can produce physical and emotional exhaustion, anxiety about future disasters and frustration associated with the constant effort required to return to normal.
Compounding disasters
Part of the challenge is that disasters increasingly do not occur in isolation.
Researchers and emergency managers often talk about these risks as cascading and compounding disasters. A flood doesn’t just damage roads; it also disrupts healthcare access, interrupts supply chains and creates long-term economic hardship. At the same time, communities may be dealing with extreme heat and housing shortages.
Climate change is contributing to many of these patterns. Heavy precipitation, extreme heat, drought and other weather-related hazards are occurring more frequently in many regions.
For communities already trying to manage a recovery, each new event adds another layer of disruption and costs.
Hidden costs of repeated recovery
One of the most important consequences of repeated disasters is the strain on social cohesion – the relationships and networks that help communities share information, coordinate resources and support one another during difficult times. Volunteers who repeatedly respond to emergencies may experience burnout.
Research examining disaster fatigue among community leaders found that people reported feeling exhausted and overwhelmed by the many decisions, lack of resources and other challenges associated with managing repeated emergencies over time.
Residents, too, can become exhausted by repeated evacuations and rebuilding cycles. Research on mental health after disasters shows that prolonged recovery demands, housing instability and uncertainty about the future can contribute to anxiety, depression and trauma-related symptoms.
Disaster fatigue does not mean weakness or failure. Communities can retain their ability to bounce back while simultaneously experiencing exhaustion. In fact, some of the most resilient communities got that way because they have had to recover from damage repeatedly.
Rethinking recovery
Repeated disasters expose weaknesses in the systems that provide aid and help with recovery, which will still be needed long after the headlines fade.
Communities often receive an immediate outpouring of support, but it can be disconnected from residents’ actual needs. Following major disasters, donations of clothing and toiletries may arrive in large quantities, yet critical needs such as housing assistance, debris removal and long-term recovery support such as childcare services or healthcare and social service support may go unmet.
Effective recovery depends not only on the generosity of the donations, but also on strategic approaches that can get the type of aid needed to the people who need it. Long-term recovery planning and coordinated recovery efforts – combining the strengths of government agencies, nonprofits, faith-based organizations and community groups – can help tap into the funding and types of assistance most needed and help communities quickly determine where the need will be greatest.
Recognizing community disaster fatigue is an important step toward building recovery systems that are as enduring as the challenges communities increasingly face.
These systems require sustained investments in people, institutions and communities. As disasters become more frequent and recovery efforts increasingly overlap with new floods, storms, heat waves, droughts and other disruptions, strengthening these systems will be crucial for successful, resilient recoveries.
This article, originally published July 13, 2026, has been updated with new flooding in Texas Hill Country.
This article is republished from The Conversation, a nonprofit, independent news organization bringing you facts and trustworthy analysis to help you make sense of our complex world. It was written by: Lee Ann Rawlins Williams, University of North Dakota
Read more:
- Millions of Americans are displaced by tornadoes, wildfires and other disasters each year ‑ who they are tells a story of vulnerability and recovery
- 4 reasons affordable housing is slow to recover after disasters like hurricanes, and what communities can do about it
- 4 urgent lessons for Jamaica from Puerto Rico’s troubled hurricane recovery – and how the Jamaican diaspora could help after Melissa
Lee Ann Rawlins Williams does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
NC auditor’s former liaison resigns amid furor over pressuring county elections board on early voting plans
by Sarah Michels, Carolina Public Press
July 13, 2026
The day after Anson County election board members chose between early voting plans, Election Director Neva Helms and Republican Board Chair Kelly Newton received a text from Dallas Woodhouse, the state auditor’s liaison with county boards of election.
“We are going to have to redo that early voting plan,” he wrote.
Woodhouse resigned Monday after a series of his suggestions to county boards became public.
[Subscribe for FREE to Carolina Public Press’ Daily, Weekend and Election 2026 newsletters.]
In late 2024, state lawmakers transferred the governor’s power to appoint county election board chairs and State Board of Elections members to the recently elected Republican state auditor, Dave Boliek. As a result, each of the state’s election boards shifted from 3-2 Democratic to Republican majorities.
Under the new law, most of election boards’ business would remain independent of the auditor’s office, with the exception of the initial appointments and budget oversight.
However, since election boards shifted, some feel like the auditor has blurred the lines of his authority. In public records, Woodhouse takes center stage in conversations with county election board members and staff about early voting plans for the 2026 election.
Early voting decisions are always ripe for drama, but in the first major election since the election boards’ party shift, tensions have escalated. So far, 18 county boards have disagreed over early voting decisions, compared to 13 nonunanimous plans in the last 2022 midterm election.
There is still time to come to an agreement before the July 24 deadline.
Anson County re-do?
In early May, Anson County Election Director Helms got an email from Woodhouse.
Woodhouse attached a proposed early voting plan, which would reallocate six Sunday voting hours from the 2022 midterm plan to the first two Saturdays of the early voting period, according to a Carolina Public Press records request. The resolution stated that the move “preserves and enhances voter access while aligning voting opportunities with historically higher-utilization days in Anson County.”
However, when the county board met, Helms provided three staff recommendations.
The first option did not include any Saturday or Sunday early voting hours, except the legally required last Saturday before Election Day. The second included a Sunday early voting day. The third was Woodhouse’s recommendation, which included two additional Saturdays from 8 a.m. to 6:30 p.m. and no Sundays.
During the June 9 meeting, the county board majority voted for the first plan, while the two board Democrats objected. As with all nonunanimous plans, Anson County’s early voting schedule was then sent to the State Board of Elections for a final decision sometime in July or August.
The next day, Woodhouse texted Helms and Republican Board Chair Kelly Newton.
“We are going to have to redo that early voting plan,” he wrote. “We simply can’t cut nearly 60 early voting hours. GOP NCSBE can’t stomach that and really neither can we.”
Newton pushed back, asking why the plan wasn’t good enough when it met state law’s minimum requirements.
Woodhouse said he thought the plan would not be approved by the State Board of Elections.
Later in the conversation, Woodhouse suggested using newly available money discovered in their budget to bring the matter back up for reconsideration.
He emphasized the importance of getting to a unanimous decision. Newton and Helms appeared hesitant, and indicated that board Democrats would not change their minds about Sunday early voting.
Woodhouse outlined a plan for Helms to approach board Democrats with a deal: we’ll give you extra Saturday hours if you vote for a unanimous plan.
“Fact is GOP voters need hours beyond 8-5 and some Saturdays is good,” Woodhouse texted.
A few weeks later, on June 26, Woodhouse reminded Newton to revise the early voting plan. Still, Newton was hesitant. She asked whether they could stick with their original plan — “the best option in my humble opinion,” he texted — and have Woodhouse’s plan as a backup.
“We need you guys to pass a revised plan,” Woodhouse responded. “No Sundays is fine but we have to have some week day hours extended and Saturday hours. we can then back up a divided plan at the state.”
The Anson County board’s Tuesday, July 14, meeting agenda includes reconsideration of the early voting plan.
Woodhouse resigned from the auditor’s office effective Monday, July 13.
In his resignation letter, he said that early voting decisions are among the most difficult local election officials make, considering every county’s unique features,challenges and expectations.
“There is rarely a perfect answer, and reasonable people frequently reach different conclusions,” he wrote.
“I am certain that my advice was not always correct. Looking back, there are recommendations I might make differently today. I certainly would have been more precise in my communications at times.”
Woodhouse said he made his recommendations with honesty and integrity, with the sole objective of helping county boards follow the law “while improving voter access and strengthening public confidence in our elections.”
State Board of Elections spokesperson Pat Gannon said State Board staff do not suggest or recommend one early voting plan over another. Woodhouse worked directly under the State Auditor and was not part of the State Board staff.
"Elected officials, candidates, political parties, advocacy groups, and everyday citizens are free to – and often do – provide recommendations about where and when to conduct early voting," Gannon said in a statement.
"State Board staff has not and will not do that, aside from informing county officials that they should be guided by principles of ensuring fair access for all voters according to their available resources."
Auditor’s office weighs in on early voting plans
Helms and Newton weren’t the only ones to receive texts, emails and calls from Woodhouse or other representatives of the auditor’s office in recent months about their early voting plans. But not many listened.
Drama ensued in Jackson County last month when one Republican election board member resigned in protest before the early voting plan meeting and another voted with Democrats in the face of what they said was pressure from the auditor’s office and other groups to exclude a Western Carolina University campus early voting site.
In Columbus County, Woodhouse texted election staff on May 27 advising them to choose three specific early voting sites for the upcoming election, in Whiteville, Chadbourn and Tabor City, according to public records shared with Carolina Public Press.
A few weeks before, the county elections chair had floated the idea of dropping from five to one early voting site based on rising costs and low voter participation, with plans to discuss in June.
“I agree 5 is overkill, but we can’t go below 3,” Woodhouse texted. “Those are the largest towns and geographically diverse. It matches some other key goals as well.”
He did not clarify what those goals were.
In a packed meeting, the Columbus County board’s majority ultimately voted for four early voting sites, while the minority insisted on keeping five. The plan will go to the State Board for a final decision. They may pick the majority plan, minority plan or choose one of their own.
The auditor’s office made suggestions in other places, too. In Cabarrus County, emails between the county election director and assistant county manager reveal that the auditor wanted an early voting site in Midland. The county is still figuring out its plans.
Woodhouse called Alamance County election chair Kevin Patrick Harrison after they passed a unanimous plan asking about a potential site in the southern part of the county. The county has not changed its plan.
In a phone call, he also told Granville County election board chair Larue Ulshafer that the auditor preferred to keep four early voting sites, despite tight county budgets, according to emails between Ulshafer and the county election director.
During a June 16 meeting, Ulshafer advocated for moving two early voting sites away from Creedmoor and downtown Oxford, places where Democrats have greater odds of winning, to more rural, northern Stovall and a location five miles south of the city. He also voted to remove another Creedmoor site altogether, which would put the county at three sites.
During the discussion, Ulshafer referred to the auditor as “the boss” and said he was working toward a “vision” he heard him describe in a Raleigh meeting.
"The boss said, 'my vision is we have free and equal voting across the county' — north, south and central — and that's what we're working towards," Ulshafer said.
Ulshafer has since resigned, and did not respond to a request for comment. During a July 15 special meeting, the board will reconsider their early voting plans.
In Randolph County, auditor’s office representative Kirk O’Steen asked election board chair Aundrea Azelton to add a site in Liberty, in the county’s northeastern corner, based on size and population growth. The board declined.
Woodhouse suggested exchanging a Sunday early voting day for a Saturday in a text to Pasquotank County chair Larry Beatty. If he did so, he would be “adding voting opportunities, saving money and giving staff much needed day off,” Woodhouse wrote.
Ultimately, Pasquotank County’s election board disagreed on whether to include two Saturdays or a Saturday and a Sunday, as well as their site location and hours. Their plan will go to the State Board.
After news media reports alleging auditor interference proliferated, Woodhouse was reassigned to a different role within the auditor’s office.
Nonunanimous early voting plans
Before Barbara Hilty was McDowell County’s election board chair, she helped recruit poll workers for the Republican Party. It was a “really, really, really hard” job, she said.
Combined with continued financial recovery needs from Hurricane Helene, Hilty feels it’s best to have only the one statutorily required Saturday of early voting.
“Saving a little bit of money right now is important in McDowell County,” she said.
Hilty did talk to Woodhouse last fall about his suggestion to add a third early voting site in the northern part of the county. Even though it might benefit Republicans, she said it’s not worth it; the northern region is mountainous and everyone who lives there has to come down to grocery shop or go to the post office anyways.
The Democratic minority preferred two or three Saturdays, which means McDowell County’s plan will go to the State Board.
Nearly all county-level disagreements involved Saturday or Sunday early voting days.
Historically, Democrats have supported Sunday voting more than Republicans. While Democrats may feel that Sunday events like Souls to the Polls benefit voters of their party, Republicans typically cite Sunday as a religious day of rest.
While it’s not as pronounced, Democrats also tend to support Saturday voting more on the grounds that it provides more options for working people. Republicans sometimes argue that North Carolina’s two-and-a-half week early voting period and no-excuse absentee voting gives people plenty of opportunity to cast a ballot without weekends.
During the 2026 primary election, 13 counties lost a day of Sunday early voting compared to the 2022 primary — six unanimously, seven after a State Board decision.
However, there were actually 69 more early voting weekend hours across the state in the 2026 primary compared to the 2022 primary, thanks to several shifts from Sunday to Saturday voting.
Iredell County board members also split over weekend hours. Board Democrat Ginky Torres said they budgeted for two Saturdays earlier in the year, but plans changed during the actual meeting to discuss early voting plans.
Republican June Reeves voted against the two-Saturday plan, saying that she preferred just one Saturday based on “fiscal responsibility,” Torres recounted.
It left a sour taste in Torres’ mouth, she said. She prefers three Saturdays because of the accessibility for working people, but typically compromises on two for the sake of having a unanimous plan that doesn’t have to go to the state, which doesn’t understand the county’s needs as well as they do.
“We put our Democrat or Republican hat at the door,” she said.
Legislature’s early voting plans
All this comes as lawmakers consider cutting North Carolina’s early voting period from 17 days to 10 or seven.
While it’s unlikely that they’ll have time to pass a law cutting early voting before the upcoming general election, legislative leaders have expressed interest in trimming down the primary election early voting period, at the very least.
In response, several House Democrats sponsored a proposed constitutional amendment that would lock in a minimum 14-day early voting period permanently, if a majority of voters agreed.
One of the bill’s sponsors, Rep. Rodney Pierce, D-Halifax, said early voting has become the way North Carolinians prefer to vote, regardless of party affiliation.
In 2024, 74% of voters cast their ballots early, for example.
“If this is the way that people have chosen to engage in our democracy, then we should try to make sure that we keep it in place and that we protect it, and that's what this amendment does,” Pierce said.
The amendment would not require Sunday voting, but would make sure it’s allowed. It would also allow the state legislature to help counties with election costs.
“It provides certainty for voters, stability for election administrators and confidence that fundamental access to early voting cannot be dramatically reduced without first asking the people of North Carolina,” Pierce said.
Editor's note: This article has been updated with new information that became available.
This article first appeared on Carolina Public Press and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
State budget advances plan to reopen Martin County hospital
by Jaymie Baxley, North Carolina Health News
July 13, 2026
Key Takeaways
- The state budget includes a combined $40 million for a plan by ECU Health to restore emergency department services in Martin County, which has been without a local hospital since 2023.
- Under the health system’s proposal, the erstwhile Martin General campus would become North Carolina’s first Rural Emergency Hospital — and the first closed facility in the nation to be reopened through the federal designation.
- ECU Health says more investment is needed to fully implement its plan.
By Jaymie Baxley
During the prayer that opened last week’s meeting of the Martin County Board of Commissioners, chairman Joe Ayers thanked God for guiding local leaders “through the process of trying to reopen health care” in the community.
His gratitude stemmed from the state budget signed into law on July 7 by Gov. Josh Stein. Listed among the document’s thousands of line items is a $25 million allocation to restore emergency department services in Martin County.
The funding represents a major victory in the county’s three-year struggle to reopen Martin General Hospital.
Decades of mounting financial losses led to the 42-bed facility’s closure in 2023, leaving residents without local access to life-saving care.
Since then, residents have had to travel to other counties for emergency treatment, prompting concerns about longer ambulance trips, delayed care during medical emergencies and the broader economic toll of losing one of the area’s largest employers.
Last year, Greenville-based ECU Health approached the county with a potential solution: The state-affiliated hospital system proposed a plan to convert the shuttered campus into a Rural Emergency Hospital — a federal designation created by Congress to help preserve access to care in communities that can no longer support a traditional hospital.
Brian Floyd, chief operating officer for ECU Health, said the money set aside in the state budget gives the project momentum to move forward.
“Bringing emergency care to Martin County is our first priority, and this funding helps put us on a path to do that,” he said in an interview with NC Health News.
Building a regional system
Unlike a full-service hospital, Rural Emergency Hospitals provide round-the-clock emergency care and outpatient services but do not admit patients overnight. Patients who need hospitalization are stabilized before being transferred to another facility.
In return, participating hospitals receive higher Medicare reimbursements and a monthly federal facility payment intended to offset the financial challenges of operating in rural communities.
While not designated as a rural emergency hospital, Atrium Health Anson, part of the Atrium Health system, has been operating in a similar fashion since 2015, replacing an aging facility and preserving access to care in that county.
North Carolina, which has a bigger percentage of rural residents than any state except Texas, has yet to see a single hospital adopt the model. More than 50 hospitals in other states have converted, but all of them had been open when they made the switch.
This means Martin General is poised to become the first closed hospital in the nation to reopen as a Rural Emergency Hospital.
For the plan to succeed, Floyd said, emergency services must be paired with more inpatient hospital beds elsewhere in the region.
"If we have just an emergency department sitting in Martin County an hour away from the next inpatient capacity, it'll fill itself with inpatients and then not have room for emergencies," he said.
To prevent that from happening, ECU Health wants to expand its hospital in neighboring Beaufort County with an inpatient bed tower capable of absorbing patients transferred from Martin County and surrounding communities.
The entire project is expected to cost roughly $220 million, a price tag that includes about $70 million to establish the Rural Emergency Hospital in Martin County and approximately $150 million for the Beaufort expansion.
With the money from the state budget and $35 million that was previously appropriated through the state's NC Care initiative, the Martin County portion of the project is mostly funded. But lawmakers approved only $15 million toward the Beaufort expansion — enough to begin planning but well short of the amount needed to build the tower.
In a news release issued after the budget’s passage, ECU Health noted that additional investment is needed to “fully implement a sustainable regional system of care model needed to improve sustainability and expand inpatient capacity for the surrounding communities.”
Long road ahead
ECU Health and Martin County officials are now shifting to the logistical work of resurrecting Martin General.
Floyd said the next step is negotiating a formal agreement to let ECU Health operate the county-owned facility. Then engineers and construction teams will assess the building to determine what repairs and upgrades are needed before emergency services can reopen.

A few other hurdles must be cleared. Floyd said North Carolina will need to establish new Medicaid policies for Rural Emergency Hospitals, given that no facility in the state currently operates under the designation.
Another challenge will be recruiting people to work at the hospital. Floyd anticipates that some former Martin General employees will apply.
"We fully expect there will be people who have worked there and live there who'll be the first ones on the list to say, 'Can we come back to work in this new facility?'" he said. "Obviously, we think that's a great thing."
But with so many boxes left to check, Floyd was reluctant to predict when the facility might actually reopen.
"I'd like to beat any date that I think we can hit," he said. "We're going to go as fast as we can to try to bring emergency care to Martin County."
In a statement, ECU Health CEO Michael Waldrum said the state budget “represents meaningful progress toward a sustainable model of care” for Martin and Beaufort counties, as well as for eastern North Carolina as a whole.
“Rural Americans are facing unprecedented challenges that continue to threaten the viability of health care in their communities,” he said. “We are grateful for the support of our state elected leaders for infrastructure funding as we pursue rural health initiatives designed to improve the health and well-being of the most vulnerable communities in North Carolina.”
The sentiment was echoed by David "Skip" Gurganus, vice chair of Martin County’s Board of Commissioners. At the end of last week’s meeting, he praised the General Assembly for being “gracious enough to grant us what we need to start the process of reopening the hospital.”
Gurganus, like his board chairman, also gave credit to a higher power.
“I am a firm believer that God has got his hand on this,” he said.
This article first appeared on North Carolina Health News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.

This county lost its hospital. Bringing it back is easier said than done
by Gwen Dilworth, Mississippi Today
July 16, 2026
BELZONI — Harmony Ball-Stribling’s path to pregnancy had been turbulent, from an endometriosis diagnosis to an arduous in vitro fertilization process and sky-high blood pressure. But as her due date approached in the summer of 2021, her health improved and those storm clouds seemed to scatter.
“It was just too perfect,” said her mother, Shenelle Ball-Green, of those calm, hot weeks.
Then, after midnight on July 5, four days shy of her scheduled cesarean section, Ball-Stribling began experiencing complications from preeclampsia, a potentially life-threatening blood pressure disorder. Speeding up to 110 mph, her husband drove her to the nearest hospital 25 miles away from their home in Belzoni, a Mississippi Delta town of about 1,900 people.
Minutes before reaching the facility, Ball-Stribling suffered a seizure in the passenger seat. Her husband pulled her from the car and performed CPR on the side of the road. It was too late. She and the couple’s unborn daughter, Harper, died on the side of U.S. Route 49.

The tragedy might have had a different outcome if the hospital in Belzoni, a five-minute drive from Ball-Stribling's home, hadn’t closed 13 years ago. Today, Humphreys County has no hospital, no emergency room, no urgent care clinic, and no county health department. It is one of more than 100 rural hospitals in the U.S. that have fully closed since 2005.
In Belzoni, self-proclaimed “The Heart of the Delta,” and its surrounding area, communities are close-knit, and Harmony’s story is well known. Now, her death has galvanized local and state leaders determined to bring a hospital back to the county that has suffered without one.
“It was a tremendous eye-opener for this community,” said state Rep. Timaka James-Jones, a Democrat who represents the district that includes Belzoni and is Ball-Stribling’s aunt. “It brought to light how we are so without.”
Poverty often shapes the health disparities Humphreys County residents experience. Approximately 1 in 7 Humphreys County residents under age 65 lack health insurance coverage, compared with about 1 in 11 people nationwide. Humphreys County also has the highest rate of Medicaid enrollment of any Mississippi county, reflecting the economic challenges many residents face. These disparities are evident in the county’s infant mortality rate, which is among the highest in the state at roughly 15 deaths for every 1,000 births.
James-Jones has watched these circumstances influence the lives — and deaths — of her loved ones. She said she wants to see a hospital reestablished before her four-year term is up in early 2028.
But that may be easier said than done. In Belzoni, local leaders hoping to restore healthcare services face a tangled web of policy challenges that are especially demanding for a small town with limited resources. Its story reflects what many healthcare policy experts warn: Once a rural community loses a hospital, bringing it back can be nearly impossible.

Humphreys County’s healthcare losses
Humphreys County Memorial Hospital opened in Belzoni in 1951 as part of a nationwide hospital building boom fueled by a Truman-era law called the Hill-Burton Act. The legislation provided billions of dollars in grants and loans to build and modernize healthcare facilities. At the time, roughly 40% of all U.S. counties had no hospital. When the building boom began to subside by 1970, all but seven counties in Mississippi had at least one hospital.
But by the 2000s, many rural hospitals in the U.S. confronted financial difficulties. Low patient volumes, an increase in outpatient care, and meager revenues left many on precarious footing. Many had high rates of uninsured patients or those covered through government programs such as Medicaid, which typically reimburse providers at lower rates than commercial insurers.
Humphreys County’s hospital was among those struggling facilities. It was burdened with millions of dollars in debts, and county officials sold it in 2008 to a private company. It was renamed the Patients’ Choice Medical Center. The hospital shut down five years later after Ray Shoemaker, the company’s CEO, was convicted on healthcare fraud charges related to another hospital he owned.
“I do hope they reopen,” Shoemaker wrote in a recent text message to Mississippi Today. “The community needs a hospital.” He said he stepped down from the company before going to prison in 2012.

In 2017, the University of Mississippi Medical Center partnered with the county supervisors and U.S. Rep. Bennie Thompson, a Democrat whose district includes Humphreys County, to secure a nearly $1 million grant from the U.S. Department of Agriculture to open an after-hours acute care clinic in Belzoni. The clinic shut down in 2020, and UMMC officials declined to say why.
G.A. Carmichael Family Health Center, a Canton-based federally qualified health center with five other locations in Mississippi, took it over but did not maintain the extended hours, again leaving Humphreys County residents without after-hours care. Other public health services in the county have closed outright. Three years ago, the county’s health department stopped providing clinical services, said Greg Flynn, a spokesperson for the Mississippi State Department of Health. The county department closed entirely last year, citing staffing shortages and low patient volumes.
In the years since the hospital closed, the county has lost a fourth of its population, falling to 7,000 people, according to census data. James-Jones said she does not believe the community can experience growth until healthcare services are reestablished.
“I don’t know how I can see us growing any other way,” she said.
‘Something’s way better than nothing’
Months after losing her daughter and unborn granddaughter, Ball-Green climbed the steps of the stately, tan, brick Humphreys County Courthouse to attend a crowded Board of Supervisors meeting.
She stood at the dais and urged the supervisors to reestablish emergency healthcare services in the county to protect other residents from the fates of her loved ones.
“I wanted to let them know at any given moment, that could be your child, your mother,” she said. “We’re a small town. Everyone knows everyone.”

She remembered the disappointment she felt when the supervisors told her there was nothing they could do. But when the board’s makeup changed after the 2023 elections, she said, she saw these attitudes shift.
Among the newly elected officials was Reggie Pinkston, who is now the president of the board and previously worked as an EMT when the hospital was open. His own family has suffered the consequences of limited healthcare access. A cousin living in Louise, a town about 20 miles south of Belzoni in the county, had a stroke in 2021 and waited an hour for an ambulance to arrive. She died two days later.
Pinkston said witnessing residents’ delays in care has made expanding access to healthcare services one of his priorities.
“We’re losing too many people in our county because of lack of healthcare,” Pinkston said.
The board enlisted several consultants to develop a strategy for expanding healthcare access and identifying funding sources to support these efforts. In late 2025, Thompson secured approximately $1 million for Humphreys County through the congressional Community Project Funding process, which allows lawmakers to request federal support for specific projects.
The funds will be used to expand services at G.A. Carmichael’s Belzoni location in a county-owned building on U.S. Route 49, Pinkston said. Expansion plans include extending its hours of operation overnight to 5 a.m., purchasing equipment, and a possible renovation of the facility. It could begin its expanded operations by September, said James Coleman Jr., the health center’s CEO.
Establishing an after-hours urgent care clinic is a starting point toward reestablishing emergency care services or a hospital, James-Jones said.
“Something’s way better than nothing,” she said.
‘Not for the faint of heart’
Despite that encouraging first step, Humphreys County faces steep obstacles to opening a hospital.
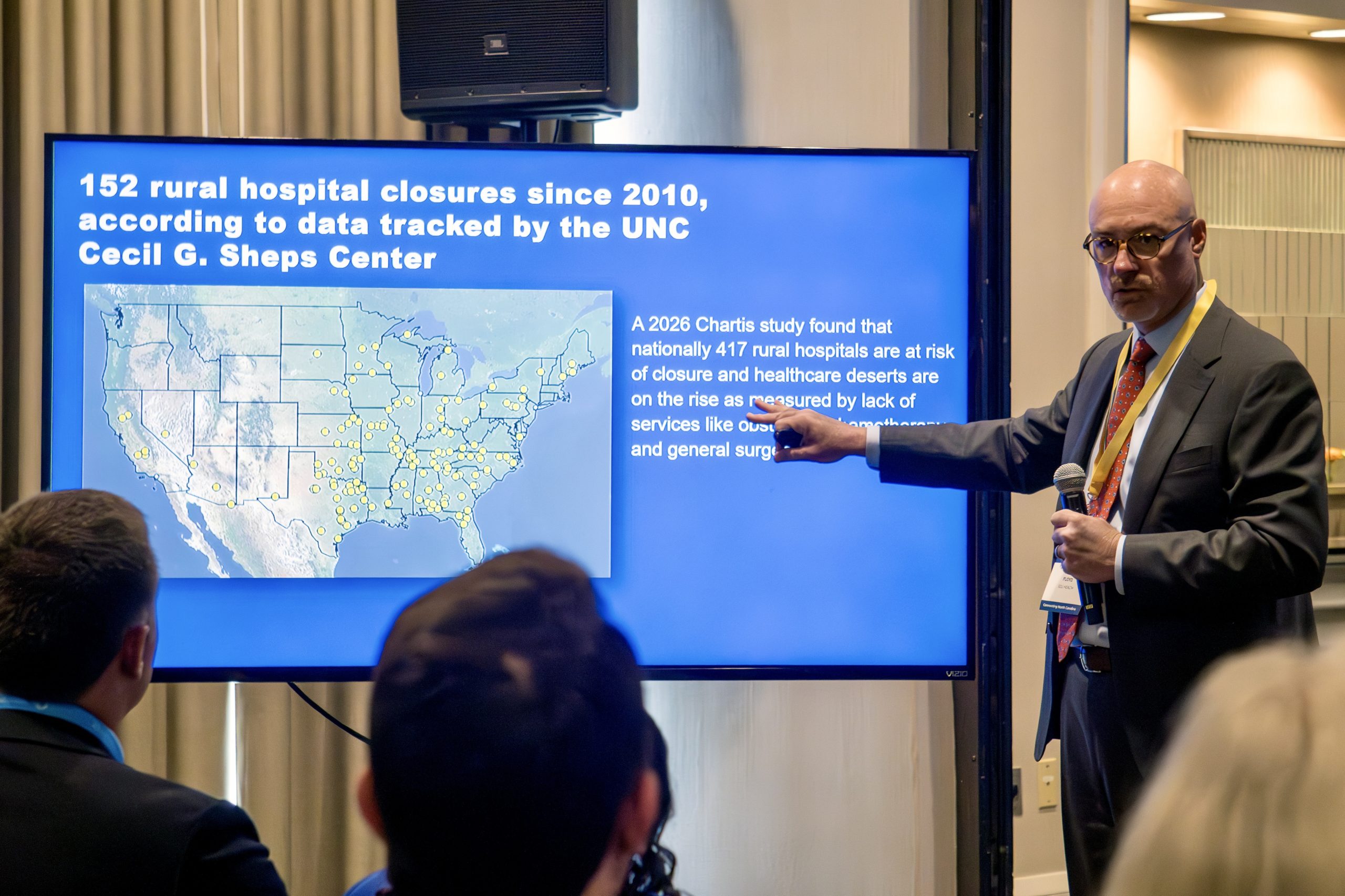
At the University of North Carolina at Chapel Hill, George Pink is a senior research fellow at the Cecil G. Sheps Center for Health Services Research and tracks rural hospital closures across the U.S. He said he’s aware of only a few communities that have successfully reopened a hospital after it closed.
“I can count that on one hand,” said Pink, who knows of roughly five such examples.
Communities face significant hurdles to reestablishing a hospital, including securing financing for construction or renovation, recruiting qualified staff, and covering substantial operating expenses during the licensing process before the facility can treat patients and generate revenue, said Brock Slabach, the National Rural Health Association’s chief operations officer and a former rural hospital administrator in southwestern Mississippi.
“Reopening a hospital is not for the faint of heart,” Slabach said. “Once they close, it’s very difficult to reopen them.”
To finance a potential hospital project in Humphreys County, local and state leaders said they plan to seek funding through the Rural Health Transformation Program, a federal initiative that will distribute $50 billion to states over five years. The federal government allocated Mississippi nearly $206 million in December for the program’s first year.
The program is meant to offset budget cuts passed into law last summer that could harm rural hospitals. Republicans’ One Big Beautiful Bill Act will cut the federal government’s Medicaid spending by $911 billion over 10 years and increase the number of uninsured people by 10 million, according to Congressional Budget Office estimates. Mississippi hospitals are projected to lose roughly $160 million annually beginning in 2029, according to Cindy Bradshaw, executive director of the Mississippi Division of Medicaid.
But according to federal guidelines, the program’s funding cannot be used for construction or major building expansions. Officials said the county will instead consider applying for funds through the program to support the recruitment of healthcare professionals.
The federal Rural Emergency Hospital designation is another way rural communities can keep emergency and outpatient services. Hospitals in that program receive over $3 million annually from the federal government and a higher Medicare reimbursement rate, but they cannot offer inpatient care.
Research by Pink’s team shows that many hospitals that converted to the model, which was established in 2023, saw an increase in profitability.
But there’s a catch. To receive the designation, a hospital must have been open in 2020, making Humphreys County ineligible. Mississippi’s junior U.S. senator, Republican Cindy Hyde-Smith, introduced legislation in 2024 to extend the cutoff to 2014, a threshold that would have still excluded Humphreys County.

James-Jones said county leaders have urged Hyde-Smith to amend the proposed legislation so Humphreys County could qualify. Hyde-Smith did not respond to a request for comment for this article.
For county leaders, the path to widening healthcare access means navigating a thicket of state and federal policies, funding streams, and regulatory hurdles.
Some recent state-level policy changes have created new opportunities for healthcare expansion in Humphreys County. In March, Republican Gov. Tate Reeves signed legislation exempting Humphreys County from Mississippi’s certificate of need requirements, which are meant to prevent unnecessary healthcare expansions.
The exemption could make the county more attractive to prospective healthcare providers. But the financial challenges that contributed to the closure of Patients’ Choice Medical Center in 2013 remain, and Mississippi lawmakers have continued to reject Medicaid expansion, limiting a potential source of reimbursement for rural hospitals and clinics.
Industry officials expect hospitals’ financial pressures to intensify as Medicaid funding cuts take effect. The latest challenge is predicting how these cuts will affect the bottom lines of these facilities and whether additional cuts will come in the future, said Richard Roberson, president and CEO of the Mississippi Hospital Association.
“If someone’s trying to run a business, they’ve got to be able to know what those numbers look like,” Roberson said. “And it’s really hard to try to project that out right now.”

‘Now I understand’
For Ball-Green, giving in to these obstacles would be a disservice to the Humphreys County residents who face health emergencies similar to the one her daughter experienced.
It has been five years since the funeral, but Ball-Green remembers it clearly.

The day was stormy, but attendees brightened the gathering by wearing yellow, Ball-Stribling’s favorite color.
As friends and family gathered to pay their respects, her mother thought back on a relative’s funeral four months earlier. At that service, Ball-Stribling sang the gospel classic “You Are My Strength” to a roomful of mourners.
“She was singing, and she looked at me,” Ball-Green said, describing a peaceful but eerie expression on her daughter’s face in that moment — a sign of something to come, though she didn’t yet know what. “She turned around, and it was just that look, you know?”
Months later, as she sat at her daughter’s funeral, she began to interpret the foreboding glance differently. She came to believe it was a sign that Ball-Stribling’s gift for helping others by sharing her story would not end with her death.
That purpose had taken shape years earlier in her work as a teacher and continued as she shared candid social media posts about her fertility struggles and IVF journey in the final months of her life. Ball-Green said the community became deeply invested in her and Harper’s story.
In the years since, this gift has endured, she said. Ball-Stribling’s story has continued to resonate throughout Humphreys County, serving as a reminder of what residents stand to lose if they do not reopen the hospital.
“I think back on when she looked back at me,” Ball Green said. “Now I understand.”
This story was produced in collaboration with KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.

Advocates, elected officials call for statewide siren system after 14 tornadoes touch down near New Orleans
by Halle Parker, Verite News New Orleans
July 15, 2026
New Orleans officials joined a coalition of community-based organizations to call for the installation of emergency siren systems across the state weeks after 14 tornadoes touched down in the greater New Orleans area from Tropical Storm Arthur.
The coalition, Louisiana Grassroots United, also asked for more tornado education as research suggests Tornado Alley — historically stretching across the Great Plains region — has shifted farther eastward than it has historically to now include Louisiana. The advocates and elected officials said while residents understand hurricanes, there’s a gap in knowledge when it comes to tornado safety.
“ At least a hurricane, you kinda have a heads up that it's on the way and it may be powerful, but a tornado is something altogether different,” said Debra Campbell, president of A Community Voice, a statewide grassroots nonprofit based in New Orleans.
Campbell and A Community Voice have pushed for siren systems in southeast Louisiana, alongside other groups, since 2022 to alert residents of emergencies, from tornadoes to flash flooding to chemical releases.

New Orleans Councilmember-at-large Matthew Willard was part of the task force that first recommended sirens to the state about four years ago, when he served in the state house. During Wednesday’s (July 15) news conference, Willard said alerts sent through phones are limited in reach and efficacy. He lived near the trail of one of the tornadoes that touched down on June 23, and he said he didn’t receive an emergency notification until 15 to 20 minutes after the tornado passed.
“ I heard it, and it was very scary, and I got the alert on my phone a few minutes later. So we have to do more,” Willard said.
Campbell said some people lack access to technology, don’t sign up for alerts or live with disabilities that make it harder to use such technology. She believed sirens would reach residents more effectively.
Willard said he plans to ask the local and state Offices of Homeland Security and Emergency Preparedness to collaborate to find money for a siren system in New Orleans once they receive a cost estimate.

In 2025, Verite News found that some companies charge $30,000 to $50,000 per siren. Councilmember Aimee McCarron, who chairs the council’s Climate and Sustainability Committee, said she will bring the discussion to her committee and explore funding options as well.
“ As climate changes, the weather patterns get more disruptive, leaving us all vulnerable to new threats,” said McCarron. “Our emergency preparedness plans should reflect this reality.”
The links between tornadoes and climate change are still being studied, but evidence suggests there could be the potential for more tornadoes outside of the traditional season for severe weather. Regardless of the cause, the data suggests the number of large tornado outbreaks and tornadoes per day have increased since 1950.
Many of the tornadoes that have occurred in the New Orleans area in recent years have occurred while it’s still dark, making them more likely to be deadly.

Campbell called for the city to consider public education campaigns such as inserts in utility bills to teach residents the difference between tornado watches and warnings, as well as where to go in their homes to stay safe. Many New Orleans homes aren’t equipped for tornadoes due to the prevalence of windows and lack of a basement.
Advocates in other parishes have spoken to their state and local representatives. Tish Taylor, program manager for the environmental group Concerned Citizens of St. John, said the sirens also could help warn her parish when dangerous flash flooding occurs.
“ Every one of our communities should have alerts. It shouldn't be specific to anyone when we are all inundated with this extreme weather. And it's not gonna stop, it's only gonna get worse,” Taylor said at the news conference.
This article first appeared on Verite News New Orleans and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.



